We use cookies to understand how you use our site and to improve the overall user experience. This includes personalizing content and advertising. Read our
Privacy Policy
Cell cytotoxicity assays are essential tools for quantifying drug-induced cell death, distinguishing between apoptotic and necrotic mechanisms, and establishing therapeutic indices in drug discovery and safety pharmacology. These assays measure membrane integrity disruption, metabolic activity loss, DNA fragmentation, and caspase activation to provide mechanistic insights into how therapeutic candidates affect cell viability. Profacgen offers comprehensive Cell Cytotoxicity Assay services utilizing LDH release, Annexin V, apoptosis, and viability detection platforms to support oncology drug screening, immunotoxicity assessment, biocompatibility testing, and biosimilar comparability.
Introduction: Assay Principle, Workflow, and Biological Meaning
Assay Principle
Cytotoxicity assays detect distinct stages and mechanisms of cell death through complementary biochemical readouts:
LDH Release: Lactate dehydrogenase is a stable cytosolic enzyme released upon plasma membrane rupture. Measurement of extracellular LDH activity (NADH-dependent reduction of tetrazolium salts) quantifies necrotic or late apoptotic membrane damage without disrupting intact cells
Annexin V Binding: Annexin V binds with high affinity to phosphatidylserine translocated from the inner to outer plasma membrane leaflet during early apoptosis. Fluorophore-conjugated Annexin V enables flow cytometric or imaging detection of apoptotic cells with intact membranes, prior to LDH release
Apoptosis Markers: Caspase-3/7 activation (DEVDase activity), PARP cleavage, and mitochondrial membrane potential loss (JC-1, TMRM) detect the programmed cell death cascade initiated by intrinsic (mitochondrial) or extrinsic (death receptor) pathways
Viability Assays: Metabolic activity (MTT, CCK-8, ATP) and membrane integrity (calcein-AM, trypan blue) measure the inverse of cytotoxicity—remaining live cell mass—providing complementary quantification of drug effect
Figure 1. Cytotoxicity assay principles. LDH release detects membrane rupture; Annexin V identifies early phosphatidylserine exposure; caspase activation reports apoptotic commitment; viability assays quantify residual live cells. (Adapted from Riss et al., 2026; Khalilzadeh et al., 2026)
Workflow
Cell Seeding: Optimized density in 96- or 384-well plates; qualified cell lines with authenticated identity and mycoplasma-free status
Compound Treatment: Serial dilution (typically 10-point, half-log increments); treatment duration matched to mechanism (24h for apoptosis, 48–72h for proliferation-dependent cytotoxicity)
Multiplex Detection: Sequential LDH release (supernatant) followed by viability (remaining cells) in same wells; parallel Annexin V/PI flow cytometry for mechanism classification
Signal Quantification: Absorbance (LDH, MTT), fluorescence (Annexin V-FITC, calcein-AM), or luminescence (caspase luminescence assay, ATP luminescence assay) on plate readers or flow cytometers
Data Analysis: IC50, LC50, and therapeutic index calculation; apoptosis/necrosis ratio from Annexin V/PI quadrant analysis; time-course kinetics for mechanism evolution
Biological Meaning
Mechanism Discrimination: Early apoptosis (Annexin V+/PI−) versus late apoptosis/necrosis (Annexin V+/PI+) versus primary necrosis (Annexin V−/PI+) guides therapeutic strategy and toxicity mitigation
Therapeutic Index: Ratio of cytotoxicity in tumor cells versus normal cells determines clinical utility; mechanism-specific cytotoxicity (e.g., TRAIL receptor expression dependence) enables targeted therapy design
Immune Effector Function: ADC, CAR-T, and bispecific antibody cytotoxicity against target-expressing cells versus off-target cells validates selective killing mechanism
Applications
Oncology drug screening: cytotoxic and cytostatic agent profiling; combination therapy synergy assessment
Immunotoxicity evaluation: off-target killing of normal tissues by immunotherapies; cytokine release syndrome prediction
Biocompatibility testing: medical device extract cytotoxicity per ISO 10993-5; nanoparticle safety assessment
LDH + Viability Same-Well: Supernatant LDH followed by ATP luminescence viability assay on remaining cells; complete cytotoxicity profile from single well
Annexin V / 7-AAD / BrdU: Triple staining for apoptosis, membrane integrity, and cell cycle position; identifies cell cycle-specific killing
Caspase Multiplex Panel: Caspase-2, -3/7, -8, and -9 selective substrates distinguishing intrinsic versus extrinsic apoptosis initiation
3D Spheroid Cytotoxicity: ATP or live/dead imaging of tumor spheroids; penetration-limited drug effects and necrotic core formation
ADCC / CDC Effector Assays: Target cell killing by antibody-dependent cellular cytotoxicity or complement-dependent cytotoxicity; LDH or calcein release with effector-to-target ratio optimization
Deliverables
Percent cytotoxicity with vehicle and positive control (Triton X-100 or staurosporine) normalization
IC50, LC50, and EC50 with 95% confidence intervals
Apoptosis mechanism classification: early apoptosis %, late apoptosis/necrosis %, viable %
Caspase activation fold-change and kinetic onset time
Therapeutic index: tumor cell IC50 / normal cell IC50 ratio
Combination index (CI) for drug synergy, additivity, or antagonism
Mechanism-Resolved Multiplexing: Simultaneous LDH, Annexin V, caspase, and viability readouts distinguishing apoptosis from necrosis and cytostasis from cytotoxicity
High-Throughput Execution: 384- and 1536-well homogeneous formats (caspase luminescence, ATP luminescence, LDH luminescence) enabling 50,000+ compound weekly screening
Immune Effector Expertise: Validated ADCC, CDC, and CAR-T cytotoxicity protocols with primary human PBMCs and NK cells as effectors
3D Tumor Model Compatibility: Spheroid and organoid cytotoxicity with penetration kinetics and hypoxic core necrosis assessment
Primary Cell and Normal Tissue Panels: Cardiomyocyte, hepatocyte, and neuronal cytotoxicity for early safety liability identification
Regulatory-Compliant Operations: GLP validation, ISO 10993-5 biocompatibility protocols, and biosimilar potency documentation
Representative Case Studies
Case 1: Multiplex Cytotoxicity Profiling Identifies Necroptosis Mechanism of a RIPK1 Inhibitor
Background:
A kinase inhibitor program targeting RIPK1 for inflammatory disease observed unexpected hepatotoxicity in preclinical studies. Standard viability assays showed dose-dependent cell killing, but could not distinguish whether the toxicity resulted from on-target necroptosis inhibition (RIPK1 blocks necroptosis, so inhibition should increase necrosis) or off-target cytotoxicity.
Our Solution:
Profacgen implemented a quadruple-readout panel: (1) ATP luminescence viability assay for total viability; (2) LDH release for membrane rupture; (3) caspase-3/7 luminescence assay for apoptosis; and (4) Annexin V/PI flow cytometry for mechanism timing. HepG2 cells were treated with the RIPK1 inhibitor, a necroptosis-inducing positive control (TSZ: TNF-α + SMAC mimetic + zVAD), and an apoptosis control (staurosporine).
Final Results:
The RIPK1 inhibitor alone showed minimal cytotoxicity (IC50 > 10 µM), but potentiated TSZ-induced killing 10-fold. In the potentiated condition, LDH release dominated (80% of total cytotoxicity) with minimal caspase activation, confirming necroptosis—not apoptosis—as the mechanism. Annexin V/PI revealed a distinct Annexin V−/PI+ population characteristic of primary necrosis. These data established that hepatotoxicity resulted from necroptosis potentiation rather than direct cytotoxicity, guiding clinical development toward lower doses in combination with necroptosis triggers rather than monotherapy, and informing patient monitoring for liver enzyme elevation.
Case 2: ADCC Cytotoxicity Potency Matching for a Trastuzumab Biosimilar
Background:
A trastuzumab biosimilar developer required functional cytotoxicity comparability data beyond binding and cell proliferation inhibition. Antibody-dependent cellular cytotoxicity (ADCC)—mediated by FcγRIIIa engagement of NK cells—is a clinically relevant mechanism of action for trastuzumab in HER2-positive breast cancer.
Our Solution:
Profacgen established a validated ADCC assay using calcein-AM-labeled SK-BR-3 cells as targets and purified human NK cells as effectors at 5:1 E:T ratio. Biosimilar and innovator were tested at 8 concentrations (0.001–10 µg/mL) with parallel binding assays (SPR) and Fc glycan profiling (mass spectrometry). Cytotoxicity was measured by calcein release after 4-hour co-incubation, with spontaneous and maximum release controls for percent-specific killing calculation.
Final Results:
The biosimilar demonstrated equivalent ADCC potency (EC50: 0.052 vs. 0.048 µg/mL; Emax: 72% vs. 74% specific killing), with 90% CI entirely within predefined equivalence margins (80–125%). SPR confirmed identical HER2-ECD affinity, and glycan analysis showed comparable fucosylation and galactosylation patterns that determine FcγRIIIa binding. The integrated cytotoxicity, binding, and glycan data package supported successful regulatory approval, with the ADCC assay incorporated into QC lot release testing.
Q: How do LDH release and viability assays differ in cytotoxicity measurement?
A: LDH release measures dead cells by detecting enzyme leakage from membrane-compromised cells into supernatant. Viability assays (MTT, CCK-8, ATP) measure live cells by metabolic activity in remaining adherent cells. LDH is preferred when compounds interfere with metabolic enzymes or when cells detach upon death. Viability assays are more sensitive for weak cytotoxicity. Profacgen recommends multiplexing both in the same well: LDH from supernatant followed by ATP luminescence viability assay on remaining cells provides complete cytotoxicity profile without well-to-well variation.
Q: Can cytotoxicity assays distinguish apoptosis from necrosis?
A: Yes, through sequential detection. Early apoptosis: Annexin V+/PI− (intact membrane, phosphatidylserine exposure). Late apoptosis: Annexin V+/PI+ (membrane permeable but caspase-activated). Necrosis: Annexin V−/PI+ (primary membrane rupture without caspase activation). Caspase-3/7 luminescence assay confirms apoptotic commitment. Necroptosis (regulated necrosis) shows RIPK1/MLKL dependence without caspase activation, confirmed by necrostatin-1 inhibition. Profacgen's multiplex panels classify mechanism in a single experiment.
Q: What causes high background in LDH release assays?
A: Common causes: (1) spontaneous LDH release from fragile cell types (primary neurons, hepatocytes); (2) serum LDH contamination in FBS lots; (3) edge effects from evaporation-induced osmotic stress; (4) mechanical disruption during pipetting; (5) extended incubation beyond optimal time. Solutions: use low-LDH serum or serum-free medium with supplements; include maximum release controls for normalization; avoid edge wells; use gentle handling protocols; optimize incubation time for each cell type. Profacgen qualifies FBS lots and implements standardized handling to maintain spontaneous release < 15% of maximum.
Q: Are cytotoxicity assays suitable for 3D cultures?
A: Yes, with modifications. 3D spheroids exhibit penetration-limited drug access, hypoxic cores, and necrotic centers that complicate endpoint interpretation. Profacgen employs: (1) ATP assays with enhanced 3D lysis reagents for spheroid penetration; (2) live/dead imaging with confocal z-stacks quantifying viable rim versus necrotic core; (3) sequential LDH release from supernatant followed by spheroid disruption for total viability; (4) size tracking by IncuCyte confluence analysis as a non-destructive proxy. Treatment durations are extended (72–168 hours) to account for slow penetration kinetics.
Q: How are cytotoxicity assays used for ADC and bispecific antibody development?
A: ADC cytotoxicity requires target antigen-dependent killing validation: (1) target-positive versus target-negative cell lines confirming selectivity; (2) bystander killing assessment using co-cultures; (3) payload mechanism confirmation (tubulin disruption for maytansinoids, DNA damage for calicheamicin); (4) Fc effector function contribution deconvolution. Bispecific antibodies (T cell engagers) require: (1) T cell activation (CD69, cytokine release) correlated with target cell killing; (2) E:T ratio optimization; (3) serial killing assessment by replenishing target cells; (4) off-target toxicity against normal tissue antigen-expressing cells. Profacgen provides integrated cytotoxicity and immune effector panels for both modalities.
Q: What is the typical project timeline for cytotoxicity assay development?
A: Standard timelines: 2–3 weeks for execution with validated protocols; 4–6 weeks for cell line selection and treatment optimization; 6–8 weeks for multiplex panel development (LDH + Annexin V + caspase); 8–10 weeks for ADCC/CDC effector assay establishment with primary cell qualification; 10–12 weeks for GLP validation. High-throughput screening: 2–3 weeks for single-point screens, 4–6 weeks for IC50 confirmation. 3D spheroid cytotoxicity: 6–8 weeks including penetration kinetics and imaging protocol optimization.
References:
Riss T, Niles A, Moravec R, Karassina N, Vidugiriene J. Cytotoxicity assays: in vitro methods to measure dead cells. In: Assay Guidance Manual. Eli Lilly & Company and the National Center for Advancing Translational Sciences; 2019. Accessed May 21, 2026. https://www.ncbi.nlm.nih.gov/sites/books/NBK540958/
Khalilzadeh B, Shadjou N, Kanberoglu GS, et al. Advances in nanomaterial based optical biosensing and bioimaging of apoptosis via caspase-3 activity: a review. Microchim Acta. 2018;185(9):434. doi:10.1007/s00604-018-2980-6
Online Inquiry
Fill out this form and one of our experts will respond to you within one business day.
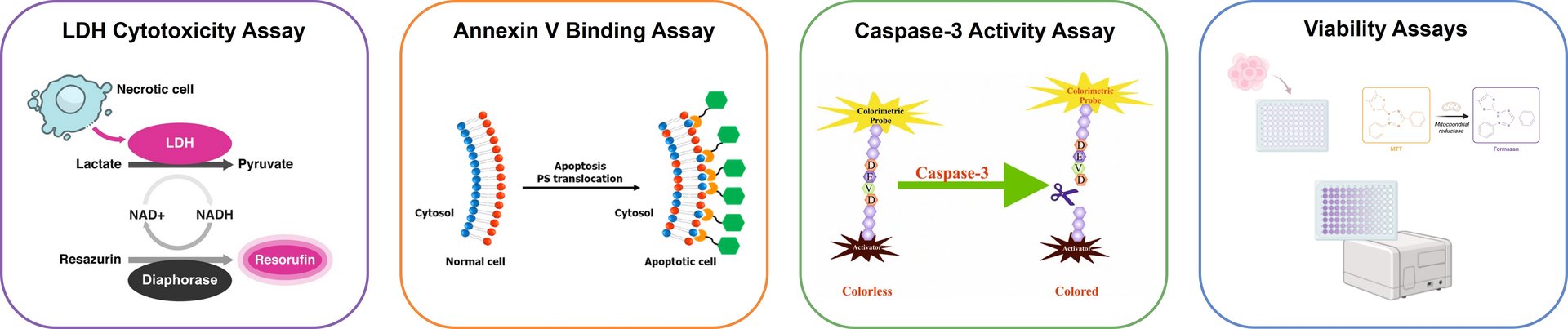 Figure 1. Cytotoxicity assay principles. LDH release detects membrane rupture; Annexin V identifies early phosphatidylserine exposure; caspase activation reports apoptotic commitment; viability assays quantify residual live cells. (Adapted from Riss et al., 2026; Khalilzadeh et al., 2026)
Figure 1. Cytotoxicity assay principles. LDH release detects membrane rupture; Annexin V identifies early phosphatidylserine exposure; caspase activation reports apoptotic commitment; viability assays quantify residual live cells. (Adapted from Riss et al., 2026; Khalilzadeh et al., 2026)