We use cookies to understand how you use our site and to improve the overall user experience. This includes personalizing content and advertising. Read our
Privacy Policy
The complement system is a tightly regulated network of over 35 plasma and cell-surface proteins that bridges innate and adaptive immunity through opsonization, inflammatory cell recruitment, and direct target cell lysis via the Membrane Attack Complex (MAC). Dysregulated complement activation contributes to the pathogenesis of chronic inflammatory disorders, autoimmune diseases, and infectious conditions, while inherited or acquired complement deficiencies confer susceptibility to recurrent infections and immune complex deposition. Profacgen offers a comprehensive suite of Functional Complement Assays designed to quantitatively assess the biological activity of each complement activation pathway independently. Our standardized, GLP-compliant platform enables precise measurement of classical, alternative, and MB-lectin pathway function, supporting drug development programs, clinical biomarker strategies, and mechanistic immunology research.
What We Offer
Profacgen provides end-to-end functional complement testing services that measure pathway-specific activity rather than simple protein abundance. Our assays distinguish between intact complement capacity and actual activation potential, delivering actionable data for therapeutic development and patient stratification.
Classical Pathway Function Assay
Quantitative assessment of C1q-initiated complement activation through C1r, C1s, C4, C2, and C3 engagement, measured by deposition of terminal pathway components on sensitized target surfaces.
Alternative Pathway Function Assay
Evaluation of C3 tick-over and Factor B/D-mediated amplification loop activity, providing specific readouts for properdin-stabilized C3 and C5 convertase function independent of classical or lectin pathway input.
MB-Lectin Pathway Function Assay
Measurement of mannose-binding lectin (MBL)-associated serine protease (MASP)-driven activation following pattern recognition of carbohydrate structures on microbial or aberrant host cell surfaces.
Comprehensive Deficiency Screening
Systematic evaluation of complement component integrity across all three pathways, identifying single or multiple component deficiencies that result in zero or reduced total complement activity.
Assay Principle and Workflow
Our functional complement assays are built on standardized hemolytic and solid-phase principles that measure the terminal output of each activation cascade. The workflow employs pathway-specific activators and neoantigen-specific detection reagents to ensure independent assessment of classical, alternative, and lectin pathway function.
Sample Preparation and Stabilization: Serum or plasma samples are collected under standardized conditions to preserve complement activity. Samples with known deficiencies or therapeutic complement inhibitors are handled with specialized protocols to distinguish exogenous suppression from intrinsic pathway defects.
Pathway-Specific Activation: Each assay well is coated with a selective activator—IgM-sensitized sheep erythrocytes for the classical pathway, rabbit erythrocytes for the alternative pathway, or mannan-coated surfaces for the MB-lectin pathway. This ensures that only the target pathway initiates the cascade.
Complement Deposition and Detection: Following incubation with diluted patient or experimental serum, deposited terminal complement components are detected using labeled antibodies specific for neoantigens generated during MAC formation (e.g., C5b-9 neoepitope). Signal intensity correlates directly with pathway functional capacity.
Quantification and Interpretation: Results are interpolated against a calibrated standard serum pool assigned 100% activity. Percentage activity is reported with reference ranges, enabling identification of complete deficiencies, partial deficiencies, or acquired consumption states.
Service Capabilities
Profacgen's functional complement platform integrates multiple assay formats and detection modalities to accommodate diverse research and clinical requirements, from high-throughput screening to regulated diagnostic development.
Capability
Description
Best Suited For
Hemolytic Function Assays
Cell-based lytic assays measuring CH50 (classical pathway hemolytic complement) and AH50 (alternative pathway hemolytic complement) using antibody-sensitized or unsensitized erythrocyte targets. Gold standard for total pathway activity assessment.
Solid-phase assays capturing pathway-specific complement deposition on coated activator surfaces, detected by enzyme-conjugated anti-C5b-9 or anti-C3b neoantigen antibodies. Higher throughput and precision than hemolytic methods.
Drug development potency testing, longitudinal clinical monitoring, preclinical pharmacodynamic studies
Nephelometric Activity Measurement
Light-scattering quantification of immune complex formation during complement activation, enabling rapid automated assessment of functional capacity in clinical laboratory settings.
High-volume clinical diagnostics, routine monitoring of complement-targeting therapies
Multiplex Pathway Profiling
Simultaneous assessment of all three pathway activities in a single sample well, with independent readouts for classical, alternative, and lectin pathway function using differential activator coatings and fluorescent detection.
Comprehensive pathway mapping, drug mechanism studies, biomarker discovery programs
Supported Targets and Pathway Components
Our functional assays assess the integrated activity of pathway-specific component cascades, with validated sensitivity to detect deficiencies or modulations in:
Terminal Pathway Components: C5, C6, C7, C8, C9 (common to all activation routes)
Regulatory Proteins: Functional impact assessment of Factor H, Factor I, C1 inhibitor, and CD55/CD59-mediated regulation
Figure 1. Overview of the complement cascade. (Hallstrom and Riesbeck, 2010)
Applications
Functional complement assays provide critical insights across therapeutic development, clinical diagnostics, and translational research:
Complement Therapeutic Potency Testing: Quantitative assessment of C3, C5, C1q, and Factor B inhibitors (eculizumab, ravulizumab, pegcetacoplan) for batch release, stability studies, and regulatory submission support.
Clinical Complement Function Monitoring: Longitudinal tracking of pathway activity in patients receiving complement-targeted therapies, enabling dose optimization, breakthrough hemolysis detection, and treatment response stratification.
Off-Target Complement Reactivity Assessment: Evaluation of unintended complement activation by biologics, nanoparticles, or medical devices, supporting immunogenicity risk assessment and regulatory safety packages.
Inherited Deficiency Diagnosis: Systematic identification of single or multiple component deficiencies (C1-C9, Factor B, Factor D, Properdin, MBL) presenting with recurrent infection, SLE-like autoimmunity, or atypical hemolytic uremic syndrome.
Autoimmune Disease Pathophysiology: Assessment of complement consumption in systemic lupus erythematosus, rheumatoid arthritis, and antiphospholipid syndrome, correlating functional depletion with disease flare activity and organ involvement.
Infectious Disease Immune Competence: Functional complement profiling in sepsis, meningococcal disease, and COVID-19 to assess consumption-mediated immunoparalysis and guide adjunctive therapeutic strategies.
Service Advantages
Pathway Isolation Integrity: Activator-specific coatings ensure classical, alternative, and lectin pathway readouts without cross-pathway interference
Standardized Hemolytic Correlation: ELISA-based results demonstrate quantitative agreement with CH50 and AH50 reference methods
Regulatory Compliance: GLP and ISO 17025-aligned protocols with full traceability for IND-enabling and diagnostic development studies
High-Throughput Automation: Validated robotic protocols for screening campaigns and large clinical cohort analysis
Flexible Assay Adaptation: Customizable sample matrices, dilution schemes, and inhibitor co-incubation protocols for specialized research requirements
Comprehensive Interpretation Support: Expert consultation on deficiency pattern recognition, therapeutic mechanism assessment, and biomarker correlation analysis
Deliverables
Each functional complement assay project includes complete analytical documentation and expert data interpretation:
Pathway-specific functional activity reported as percentage of standard serum reference (classical, alternative, MB-lectin)
Total hemolytic complement activity (CH50/AH50 equivalents) where applicable
Intra- and inter-assay precision metrics (CV) and assay acceptance criteria
Standard curve parameters and goodness-of-fit statistics
Raw absorbance/fluorescence values and intermediate calculations upon request
Clinical or preclinical interpretation report with pathway-level insights
GLP-compliant study reports with full audit trails for regulated submissions
Case 1: Classical Pathway Potency Assay for Anti-C1q Therapeutic Antibody Development
Background:
A pharmaceutical company developing a first-in-class anti-C1q monoclonal antibody for systemic lupus erythematosus (SLE) required a standardized functional potency assay for lot release and stability testing. The therapeutic mechanism depended on complete classical pathway blockade without affecting alternative or lectin pathway function, necessitating pathway-specific functional readouts rather than total complement consumption measurements.
Our Solution:
Profacgen developed a customized classical pathway function assay using IgM-sensitized target cells with a C5b-9 neoantigen detection endpoint. The assay was optimized to demonstrate complete classical pathway inhibition at therapeutic antibody concentrations while preserving >90% alternative and lectin pathway activity. We established system suitability criteria, reference standard qualification, and intermediate precision protocols in compliance with ICH Q2(R1) guidelines.
Final Results:
The validated assay demonstrated a dose-dependent classical pathway inhibition curve with an EC50 within 15% across three independent qualification runs. The assay was transferred to the client's QC laboratory with full documentation, enabling GMP lot release testing and supporting the therapeutic's progression to Phase II clinical trials.
Case 2: Three-Pathway Functional Profiling for Complement-Mediated Adverse Events in Gene Therapy
Background:
A gene therapy developer observed unexpected complement activation in non-human primate studies following systemic vector administration, presenting as thrombocytopenia and systemic inflammation. Standard component-level testing showed normal C3 and C4 concentrations, failing to capture the dynamic complement consumption occurring during acute infusion reactions. The client needed real-time functional pathway profiling to identify the activation mechanism and guide vector engineering.
Our Solution:
Profacgen implemented a multiplex functional complement panel measuring classical, alternative, and lectin pathway activity in serial serum samples collected pre-dose, during infusion, and post-infusion. The assay format enabled simultaneous pathway comparison within a single sample volume, critical for limited NHP specimen availability. We correlated functional depletion patterns with clinical biomarkers and histopathology findings to map the activation trigger.
Final Results:
Functional profiling revealed selective alternative pathway hyperactivation within 30 minutes of vector exposure, driven by spontaneous C3 tick-over on the viral capsid surface. This mechanistic insight directed the client toward capsid modification strategies that reduced alternative pathway engagement by 80% in subsequent studies, clearing the path for IND-enabling toxicology and first-in-human trial design.
Q: What is the difference between functional complement assays and component quantification assays?
A: Functional assays measure the biological activity of complement pathways—specifically their capacity to activate and generate terminal complexes like MAC. Component quantification assays (such as antigen-level ELISAs or nephelometry) measure protein concentration regardless of functional integrity. A component may be present at normal levels but functionally inactive due to mutations or inhibitory antibodies; conversely, consumption during active disease may deplete functional capacity before total protein drops significantly. Functional assays therefore provide complementary and often more clinically relevant information.
Q: Can a single deficient complement component completely abolish pathway activity?
A: Yes. The complement cascade is a sequential proteolytic activation pathway where each component depends on the preceding one. If any essential component is absent or non-functional—whether C1q in the classical pathway, Factor B in the alternative pathway, or MBL in the lectin pathway—the entire downstream cascade halts. Our assays detect this as zero or severely reduced pathway-specific activity, enabling precise deficiency localization when combined with component-level testing.
Q: How do functional complement assays support complement inhibitor drug development?
A: Functional assays serve as critical potency and pharmacodynamic tools throughout drug development. During lead optimization, they quantify pathway suppression by candidate inhibitors. For clinical translation, they monitor patient complement activity to confirm target engagement, optimize dosing, and detect breakthrough activation. For regulatory submissions, standardized functional assays provide mechanistic evidence of therapeutic effect and support batch release testing for complement-targeted biologics.
Q: What sample types are compatible with functional complement assays?
A: Serum is the preferred matrix for functional assays because it retains full complement activity with all components present in their native concentrations. EDTA and citrate anticoagulants chelate calcium and magnesium, which are essential cofactors for multiple complement proteases, thereby inhibiting activation and invalidating functional readouts. Heparin may also interfere with certain components. We provide detailed serum collection and handling protocols to ensure assay validity.
Q: How do you distinguish between pathway-specific inhibition and total complement depletion?
A: By testing all three pathways independently in parallel. If only the classical pathway is suppressed while alternative and lectin pathways remain normal, the defect is localized to classical-specific components (C1q, C1r, C1s, C4, C2). If all three pathways show reduced activity, the deficiency likely involves a terminal component (C5-C9) or a common upstream element such as C3. This pattern recognition enables efficient differential diagnosis and mechanistic interpretation.
Q: What is the typical turnaround time for functional complement pathway profiling?
A: Standard turnaround for the three-pathway functional panel is 2–3 weeks from sample receipt. Expedited processing is available for time-critical clinical or preclinical studies. Large-scale screening campaigns and GLP-compliant validation studies are scheduled with dedicated project timelines and milestone reporting. Custom assay development for novel inhibitors or non-standard matrices typically requires 4–6 weeks for optimization and qualification.
References:
Brandwijk RJMGE, Michels MAHM, Van Rossum M, et al. Pitfalls in complement analysis: A systematic literature review of assessing complement activation. Front Immunol. 2022;13:1007102. doi:10.3389/fimmu.2022.1007102
Hallström T, Riesbeck K. Haemophilus influenzae and the complement system. Trends in Microbiology. 2010;18(6):258-265. doi:10.1016/j.tim.2010.03.007
Online Inquiry
Fill out this form and one of our experts will respond to you within one business day.
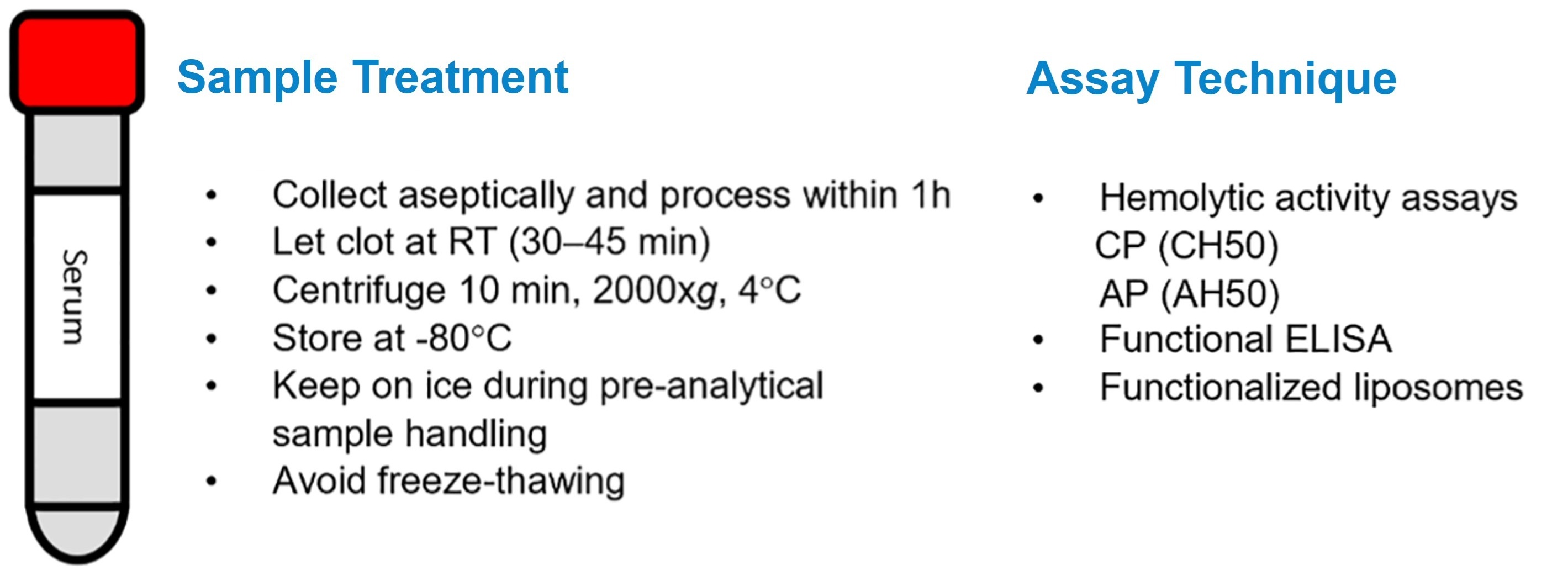
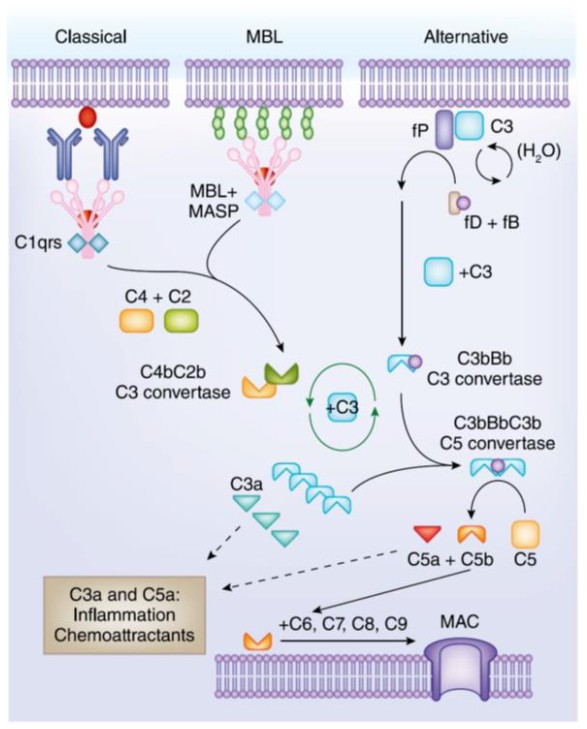 Figure 1. Overview of the complement cascade. (Hallstrom and Riesbeck, 2010)
Figure 1. Overview of the complement cascade. (Hallstrom and Riesbeck, 2010)